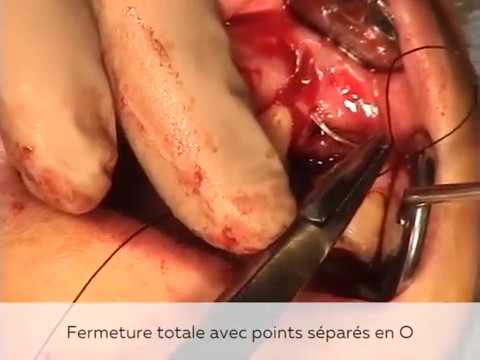
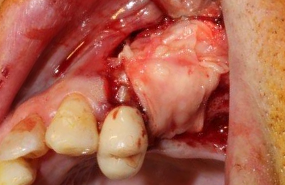
Voici une liste d’instruments indispensables pour commencer à poser des implants :
Ciseaux
Décolleur
Ecarteu…









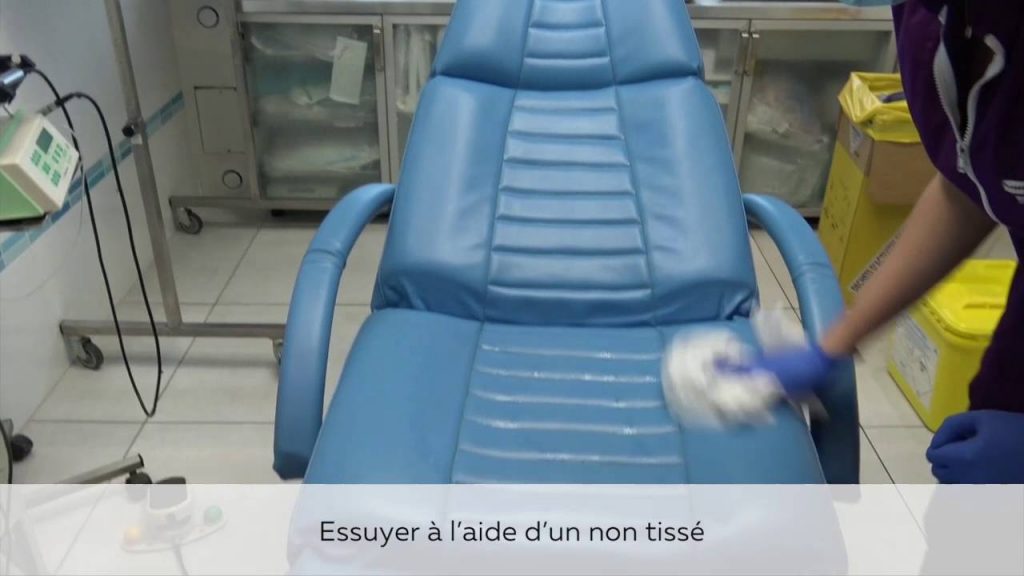








Loin de la « chasse gardée » qu’elle était il y a une dizaine d’années, la chirurgie dentaire n’est plus réservée aux spécialistes. Les chirurgiens-dentistes se heurtent pourtant souvent à des problématiques nouvelles pour eux et se posent de nombreuses questions. Dans l’Academy, portail scientifique gratuit et complet, HYGITECH vous accompagne sur tous les sujets d’intérêt : Vidéos de cas cliniques, communication avec le patient, réglementation, gestion de la traçabilité, liens utiles